بعض النصائح في تشخيص وعلاج ضيق فتحة حلمة الإثنا عشر في مرضي الحصوات الصغيرة في المرارة :
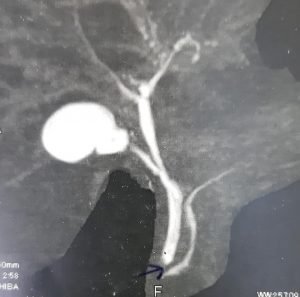
هذه الصور والفيديو توضح ضيق في فتحة حلمة الإثنا عشر لحالة تعاني من حصوات دقيقة في المرارة والفيديو يوضح إستخدام منظار القنوات المرارية لتصريف السائل المراري وهذا هام قبل إجراء عملية إستئصال المرارة بالمنظار.
وإجراء المنظار في بعض هذه الحالات قد يكون صعبا ومحفوفا بالمخاطر ويحتاج لخبرة ومهارة ولكنه ضروري قبل عملية إستئصال المرارة بالمنظار للتأكد من نوع الضيق وعلاجه و المتابعة بعد ذلك.
والشافي هو الله والحمد لله رب العالمين.
Papillary stenosis and biliary microliths : Case report and tips in diagnosis and treatment:
These are the MRCP images and ERCP videos for a 41 year old Male Patient who presented with history of Chronic calcular cholecystitis with mild jaundice with mildly elevated serum bilirubin and mildly elevated alkaline phosphate and GGT.
The Patient has undergone previous three trials of ERCP in another University hospital Endoscopy centre, but failed due to unsuccessful cannulation of the CBD due to papillary stenosis as has been mentioned in the ERCP reports.
The Patient was referred to us to do ERCP as the surgeons refused to do Laparoscopic cholecystectomy with slightly elevated serum bilirubin and alkaline phosphate and GGT.
During ERCP there was tight papillary stenosis and the papilla was small. During ERCP limited needle knife papillotomy was done for Successful selective cannulation of the CBD followed by Standard Endoscopic shincterotomy and sweeping of the CBD with a balloon with free flow of bile as seen in the videos.
The key messages are :
Recently, there is increased frequency of calcular cholecystitis with multiple small stones and microliths and sludge in the gallbladder with possible increased frequency of passage of biliary microliths and biliary sludge into the CBD and into papillary opening to the duodenum.
The passage of these microliths and biliary sludge could initiate subclinical attacks of ascending cholangitis with microscopic injury of the mucosa of the papillary opening initiating papillary stenosis .
In Patients with papillary stenosis, ERCP should be done to verify the pathology and to exclude papillary tumour and to achieve free biliary drainage before embarking on Laparoscopic cholecystectomy.
However, in these cases, ERCP is usually difficult and may be risky in and needs experience. A limited precise needle knife papillotomy is commonly needed to do selective CBD cannulation followed by Standard shincterotomy before sweeping of the CBD with a balloon.
I don’t prefer to put a plastic stent except when necessary, as plastic stents may initiate inflammatory reaction in the CBD with potential risk of recurrent fibrosis of the papilla especially if the papilla is small.
These cases may need follow up MRCP for further evaluation and management.
Thanks to Allah.